The idea was suggested to me (by my MD) that a blog/diary might help me feel better by venting my frustrations and struggles with Gastroparesis. Also, I hope I can help others who may have the same thing through my own experiences.
For more information, please email: emilysstomach[at]gmail.com or follow on Twitter: http://twitter.com/emilysstomach or like us on Facebook: http://www.facebook.com/emilysstomach or Instagram: http://www.instagram.com/emilysstomach
Copyright
“You agree that you will not modify, copy, reproduce, sell, or distribute any content in any manner or medium without permission."
Monday, July 15, 2019
Per Oral Endoscopic PyloromyotomyImag (POP) Surgery, GPOEM, and ERCP
I have had this subject saved to write about since March of this year. Life has just gotten in the way, so I've been unable to complete the article like I wanted to. However, I wanted to do some research today on the subject, now that I have had friends who have had it done. I want to talk about the
Per oral endoscopic pyloromyotomy (hereto referred as the POP procedure and GPOEM) and ERCP. I will discuss and share my research about the POP procedure first, but I have written about it in the past. You can find the article I have written on POP/GPOEM here:https://www.emilysstomach.com/2017/06/gpoem-what-is-it-and-how-does-it-help.html
"Innovative Endoscopy Procedure for Gastroparesis Is Safe and Feasible
Gastroparesis, delayed gastric emptying in the absence of mechanical obstruction, is a debilitating and chronic digestive disease affecting 5 million people in the U.S. Typically, medical therapies, intrapyloric injections of botulinum toxin, gastric electrical stimulation therapy and surgical open or laparoscopic pyloroplasty are utilized to manage the disease.
Still, it is a frustrating condition for patients and physicians alike, and until recently these medical and surgical procedures have been largely unsuccessful in resolving the disease’s symptoms or have been associated with complications. According to Cleveland Clinic general surgeon John H. Rodriguez, MD, however, a new, minimally invasive endoscopy therapy, per oral endoscopic pyloromyotomy (POP), has recently shown great promise as an alternative to surgical pyloroplasty for these patients.
Dr. Rodriguez explains that POP has been described in small case reports since 2013 and was first performed at Cleveland Clinic in January 2016. Since that time, he and his colleagues have conducted a prospective study of the technique, and recently published results in Surgical Endoscopy on the first 47 subjects (although to date they have performed almost 100 cases).
The POP study design
From January 2016 to January 2017, prospective patients who were suspected of having gastroparesis were evaluated by a multidisciplinary team comprised of a psychiatrist, dietitian, gastroenterologist and four surgeons specializing in minimally invasive techniques. Prior to having the procedure, a four-hour, non-extrapolated gastric-emptyingscintigraphy study was performed on all subjects, who subjectively rated their symptoms on the Gastroparesis Cardinal Symptom Index (GCSI). Subjects repeated the GCSI at three months after POP.
Of the 47 patients, 27 (57.4 percent) were classified as having idiopathic gastroparesis, 12 (25.6 percent) as having diabetic gastroparesis and eight (17 percent) as having postsurgical gastroparesis. The majority of the patients (87.2 percent) had been treated with one or more previous interventions for their symptoms, such as placement of an enteral feeding tube or a gastric pacer or botulinum toxin injection.
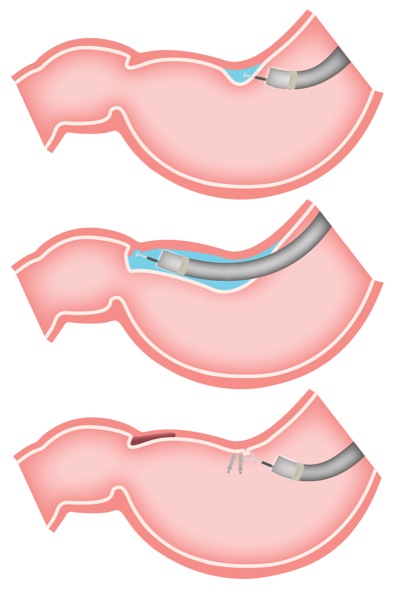
Image Source:HERE.Per-oral pyloromyotomy is a minimally invasive, lower-risk method of disrupting the pylorus that has been shown to improve gastroparesis symptoms.
The POP procedure was performed in the operating room under general anesthesia. Patients stayed in the hospital overnight after the POP procedure and an upper gastrointestinal (GI) series was performed to assess emptying through the pylorus and to check for unrecognized perforations. At discharge, patients were instructed to follow a liquid diet for two weeks and to take anti-acid therapies (sucralfate and a proton pump inhibitor) for four weeks. A repeat gastric-emptying study was performed at three months post-procedure.
The POP procedure produced statistically significant objective and subjective improvements in gastroparesis symptoms at 30 days and three months after treatment. Prior to the procedure, the average percentage of retained food at four hours was 37 percent and the average GCSI score was 4.6. After POP, the retained food percentage was reduced to 20 percent and the GCSI score to 3.3.
One patient died within 30 days of the POP procedure, but his death was unrelated to the surgery. “The procedure is very safe,” says Dr. Rodriguez, “and there were no procedure-related adverse events, including gastric or duodenal ulcer, intraluminal hemorrhage or gastric dumping syndrome.” There were also no repeat surgeries or hospitalizations related to the POP procedure.
A first-line treatment option
“This procedure has dramatically changed our practice at the Cleveland Clinic, and has become our first-line treatment option for medically refractive gastroparesis in well-selected patients,” Dr. Rodriguez says.
According to Matthew D. Kroh, MD, head of the research group and Chief of the Digestive Disease Institute at Cleveland Clinic Abu Dhabi, “POP is an attractive option for patients who in the past would have been offered surgical therapy because it is less invasive. This endoscopic procedure results that are similar to the best alternatives, without the morbidity associated with surgical access, and has a short recovery time.” Dr. Rodriguez adds that “because of its safety profile, we are able to apply POP more broadly than we could apply surgical interventions.”
Dr. Rodriguez reports that Cleveland Clinic has taken the lead in the U.S. with the POP procedure, but because GI motility is so complex and gastroparesis fairly common, he expects to see the technique become more widespread as more experience aggregates on its long-term safety and effectiveness."
"Early human experience with Per-Oral Endoscopic Pyloromyotomy (POP)
Eran Shlomovitz, MD, Radu Pescarus, MD, Ahmed Sharata, MD, Kevin M Reavis, MD, Christy M Dunst, MD, Lee L Swanstrom, MD. Providence Portland Medical Center, The Oregon Clinic..
Introduction:
Gastroparesis, a condition characterized by delayed gastric emptying, and a constellation of symptoms including nausea, vomiting, early satiety and bloating, is a debilitating condition. A variety of surgical options are available including pyloroplasty and pyloromyotomy. Although these have been shown to be effective they are associated with surgical trauma. We hypothesize that an endoscopic submucosal myotomy technique can be applied to endoscopically divide the pyloric sphincter, provide the benefits of a natural orifice procedure and improve gastric emptying in gastroparetic patients.
Methods and procedures:
Endoscopic per-oral pyloromyotomy (POP) was performed in four female patients ages 65, 59, 33 and 32 years old. All patient underwent a complete pre-operative work-up including upper endoscopy, gastric emptying study as well as a pH study and esophageal manometry if a concomitant fundoplication was performed. Three procedures were performed under laparoscopic guidance as patients required other concurrent laparoscopic procedures (see table). In one patient the procedure was fully endoscopic. The myotomy was performed by a technique similar to the one utilized in the POEM procedure. After the creation of a mucosotomy, a submucosal tunnel is established up to the duodenal bulb followed by a myotomy of the circular fibers of the pylorus. The mucosotomy is subsequently closed with clips.
Results:
Endoscopic per-oral pyloromyotomy was technically successful in all four cases and patients were discharged home on post operative day 2 or 3. There were no immediate procedural complications. One patient presented to the hospital 2 weeks post procedure with an upper GI bleed necessitating transfusions. On endoscopy a 1cm ulcer was found in the pyloric channel and an exposed vessel was clipped. The patient was subsequently discharged home on high dose proton pump inhibitors. Three month follow-up nuclear medicine gastric emptying studies (GES) are available for 3 of the 4 patients. Normalization of gastric emptying studies was demonstrated in 2 patients. Patient 3 showed improved gastric emptying half life, but unchanged residual activity at 4hrs.
Concomitant procedure
Operative time
Blood loss
Pre-op GES
Post-op GES
Patient 1
65 F
Cholecystectomy
102 min
Minimal
Half life: 150min
Residual at 4hrs: 29%
Half life: 36min
Residual at 4hrs: 0%
Patient 2
59 F
Redo- PEH repair and Nissen
295 min
100 cc
Half life: 90min
Residual at 4hrs: 14%
Half life: 18min
Residual at 4hrs: 0%
Patient 3
33 F
Nissen
231 min
Minimal
Half life: 160-170min
Residual at 4hrs: 15%
Half life: 70-90min
Residual at 4hrs: 14%
Conclusion:
Endoscopic pyloromyotomy is a technically feasible and potentially much less morbid endoscopic surgical procedure. Early follow-up suggests objective improvement in gastric emptying. Further long-term follow-up and additional clinical experience is required to establish the role of this technique in the management of gastroparesis."
Now, I want to discuss ERCP. I have had this procedure done to me, personally, and it helped me a great deal. I had my ERCP done in 2012, when I was first diagnosed with Gastroparesis. The doctors had to place a stent in my bile duct of my liver because it was not draining bile properly. You can read more about my personal experiences in my earlier blog articles:
I did develop pancreatitis after the procedure, which can be a side effect. That was a very painful experience. However, I want to research ERCP for those of you whose doctors may have suggested it, for those of you curious about it, and for those of you who might not know about the procedure itself.
There is a wonderful video with an explanation of the procedure made bySages,
This talk was presented at the 2018 SAGES Meeting/16th World Congress
of Endoscopic Surgery by Heidi J Miller during the When Bad Things
Happen to Good People – Endoscopy: Being FLEXible on April 14 2018
Endoscopic retrograde cholangiopancreatography (ERCP) is a procedure that combines upper gastrointestinal (GI) endoscopy and x-rays to treat problems of the bile and pancreatic ducts.
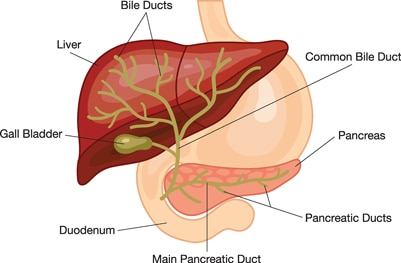
What are the bile and pancreatic ducts?
Your bile ducts are tubes that carry bile from your liver to your gallbladder and duodenum. Your pancreatic ducts are tubes that carry pancreatic juice from your pancreas to your duodenum. Small pancreatic ducts empty into the main pancreatic duct. Your common bile duct and main pancreatic duct join before emptying into your duodenum.
Why do doctors use ERCP?
Doctors use ERCP to treat problems of the bile and pancreatic ducts.
Doctors also use ERCP to diagnose problems of the bile and pancreatic
ducts if they expect to treat problems during the procedure. For
diagnosis alone, doctors may use noninvasive tests—tests that do not
physically enter the body—instead of ERCP. Noninvasive tests such as
magnetic resonance cholangiopancreatography (MRCP)—a type of magnetic resonance imaging (MRI) —are safer and can also diagnose many problems of the bile and pancreatic ducts.
Doctors perform ERCP when your bile or pancreatic ducts have become narrowed or blocked because of
gallstones that form in your gallbladder and become stuck in your common bile duct
To prepare for ERCP, talk with your doctor, arrange for a ride home, and follow your doctor’s instructions.
Talk with your doctor
You should talk with your doctor about any allergies and medical
conditions you have and all prescribed and over-the-counter medicines,
vitamins, and supplements you take, including
nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen
Your doctor may ask you to temporarily stop taking medicines that
affect blood clotting or interact with sedatives. You typically receive
sedatives during ERCP to help you relax and stay comfortable.
Tell your doctor if you are, or may be, pregnant. If you are pregnant
and need ERCP to treat a problem, the doctor performing the procedure
may make changes to protect the fetus from x-rays. Research has found
that ERCP is generally safe during pregnancy.1
Arrange for a ride home
For safety reasons, you can’t drive for 24 hours after ERCP, as the sedatives or anesthesia used during the procedure needs time to wear off. You will need to make plans for getting a ride home after ERCP.
Don’t eat, drink, smoke, or chew gum
To see your upper GI tract clearly, you doctor will most likely ask
you not to eat, drink, smoke, or chew gum during the 8 hours before
ERCP.
How do doctors perform ERCP?
Doctors who have specialized training in ERCP perform this procedure at a hospital or an outpatient center. An intravenous
(IV) needle will be placed in your arm to provide a sedative. Sedatives
help you stay relaxed and comfortable during the procedure. A health
care professional will give you a liquid anesthetic to gargle or will
spray anesthetic on the back of your throat. The anesthetic numbs your
throat and helps prevent gagging during the procedure. The health care
staff will monitor your vital signs and keep you as comfortable as
possible. In some cases, you may receive general anesthesia.
You’ll be asked to lie on an examination table. The doctor will carefully feed the endoscope down your esophagus, through your stomach,
and into your duodenum. A small camera mounted on the endoscope will
send a video image to a monitor. The endoscope pumps air into your
stomach and duodenum, making them easier to see.
During ERCP, the doctor
locates the opening where the bile and pancreatic ducts empty into the duodenum
slides a thin, flexible tube called a catheter through the endoscope and into the ducts
injects a special dye, also called contrast medium, into the ducts through the catheter to make the ducts more visible on x-rays
uses a type of x-ray imaging, called fluoroscopy, to examine the ducts and look for narrowed areas or blockages
The doctor may pass tiny tools through the endoscope to
insert stents—tiny tubes that a doctor leaves in narrowed ducts
to hold them open. A doctor may also insert temporary stents to stop
bile leaks that can occur after gallbladder surgery.
The procedure most often takes between 1 and 2 hours.
What should I expect after ERCP?
After ERCP, you can expect the following:
You will most often stay at the hospital or outpatient center
for 1 to 2 hours after the procedure so the sedation or anesthesia can
wear off. In some cases, you may need to stay overnight in the hospital
after ERCP.
You may have bloating or nausea for a short time after the procedure.
You may have a sore throat for 1 to 2 days.
You can go back to a normal diet once your swallowing has returned to normal.
You should rest at home for the remainder of the day.
Following the procedure, you—or a friend or family member who is with
you if you’re still groggy—will receive instructions on how to care for
yourself after the procedure. You should follow all instructions.
You will receive instructions on how to care for yourself after ERCP. You should follow all instructions.
Some results from ERCP are available right away after the procedure.
After the sedative has worn off, the doctor will share results with you
or, if you choose, with your friend or family member.
If the doctor performed a biopsy, a pathologist will examine the biopsy tissue. Biopsy results take a few days or longer to come back.
What are the risks of ERCP?
The risks of ERCP include complications such as the following:
pancreatitis
infection of the bile ducts or gallbladder
excessive bleeding, called hemorrhage
an abnormal reaction to the sedative, including respiratory or cardiac problems
perforation in the bile or pancreatic ducts, or in the duodenum near the opening where the bile and pancreatic ducts empty into it
tissue damage from x-ray exposure
death, although this complication is rare
Research has found that these complications occur in about 5 to 10 percent of ERCP procedures.2 People with complications often need treatment at a hospital.
As always, please discuss these procedures with your doctors. This is just research I have compiled but it does not take the place of a doctor's expertise or advice.
Endoscopic — Refers to a tool called an
endoscope, a long, thin (about the width of your little finger),
flexible tube with a camera on the end.
Retrograde — Refers to the direction (backward)
in which the endoscope injects a liquid for X-rays of parts of the GI
tract called the bile duct system and pancreas.
Cholangio — Refers to the bile duct system.
Pancreatography — Refers to the pancreas.
The process of taking these X-rays is known as cholangiopancreatography.
ERCP can help find the cause of jaundice (when your skin and/or the whites of your eyes turn yellow) or pancreatitis, which is inflammation (swelling and redness) of the pancreas that is often caused by gallstones or alcohol abuse. ERCP can also treat some of those issues.
Using tools passed through the endoscopic tube, your doctor can
inject dye to light up organs under X-rays. This provides a clear view
of your pancreas, pancreatic duct, bile duct system, gallbladder and
duodenum (the first portion of the small intestine).
ERCP is an endoscopic procedure used to inject dye into the bile and pancreas ducts. X-ray pictures are then taken.
ERCP can see if there is a blockage or narrowing in your biliary or pancreatic ducts caused by stones, tumors or scarring.
ERCP is frequently performed to find the cause of abnormal
liver-chemistry tests and to follow up on an abnormal ultrasound, CT
scan or MRI exam.
During an ERCP, if any blocks are found, tools can be passed through to relieve the block. Stones can be removed from the common bile duct or pancreatic duct and blocks can be dilated, biopsied and/or stented.
ERCP can relieve jaundice (when your skin and/or the whites of your eyes turn yellow) caused by blocked bile ducts.
ERCP can help find the cause of pancreatitis, inflammation (swelling and redness) of the pancreas, and prevent future attacks.







No comments:
Post a Comment